internal medicine and internal medicine subspecialty guidelines
Disparities in Functional Impairment and Physical Therapy Referrals for Hospitalized Patients
Maylyn Martinez, MD, MSc , Rachel Baccile, MPP, Monica Peek, MD, MPH ,
Vineet Arora, MD, MAPP and David Meltzer, MD, PhD
Research Objective:
To assess differences by race and social risk in functional outcomes and physical therapy referrals for patients on inpatient medicine services.
Study Design:
A cross-sectional study was conducted at a large tertiary academic hospital. Baseline characteristics were compared using chi-squared or t-tests. Regression analysis was used to test for the association of Black race with a) receipt of an inpatient PT consult controlling for age, sex, length of stay, admission mobility score, and mobility change (discharge mobility score - admission mobility score); b) hospital-associated disability (HAD) development controlling for above covariates plus PT referral and excluding mobility change; and c) mobility change using above covariates. We adjusted for social disadvantage at the neighborhood level using the Area Deprivation Index (ADI). For the effect of Black race on mobility change we performed a mediation analysis to assess the direct effect of race when accounting for PT referral as a mediator. We performed subanalyses by age (< 65 vs ≥ 65), functional impairment on admission, and social disadvantage (high vs low).
Population Studied:
Patients admitted for > 48 hours on inpatient medicine services between 1/1/18 – 5/6/22.
Principal Findings:
Of the 10,647 admissions analyzed, the majority of patients were Black (82%). Black patients were younger (61 vs 62 years old), more likely to be male (53% vs 42%), to reside in a neighborhood with high social disadvantage (37% vs 13%) and had lower mobility scores at admission (18 vs 19) and discharge (19 vs 20).
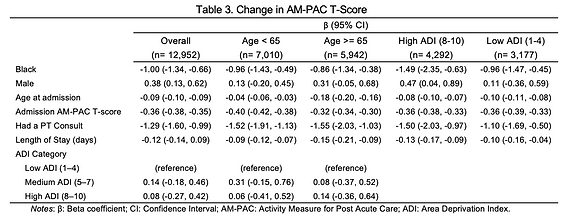
In unadjusted analyses, there was no statistically significant difference in rates of inpatient PT referrals, HAD, or mobility change by race or social risk. In adjusted analyses, Black race was associated with a negative effect on
mobility change during hospitalization [β -0.96; 95% CI (-1.28, -0.64)] with the strongest effect among those with high social disadvantage [β -1.49, 95% CI (-2.35, -0.63)]. The indirect effect of Black race through the mediator (PT referral) was 0.03 [95% CI (0.01, 0.06)], making the total effect of race -0.93 [95% CI (-1.25, -0.600)]. Black race was not otherwise associated with receipt of a PT referral except in those < 65 [OR 0.73; 95% CI (0.64, 0.84)]. Black race was associated with higher odds of HAD [OR 1.37, 95% CI (1.08, 1.74)] with a
stronger association for those ≥ 65 [OR 1.67, 95% CI (1.21, 2.30)]. In subanalyses of the highest and lowest social disadvantage, there was no significant association between Black race and HAD or PT referrals.
Conclusions:
Our findings suggest Black patients and those with social disadvantage on inpatient medicine services have poorer functional outcomes. These outcomes were not explained by differences in rates of PT referrals.
Implications for Policy or Practice:
Clinicians should emphasize physical therapy during hospitalization in these at-risk patient populations. We are using these results to inform the development of an unbiased HAD risk prediction tool.
Disparities in Post-Acute Physical Therapy
Referrals and Utilization
Maylyn Martinez, MD, MSc , Rachel Baccile, MPP , Monica Peek, MD, MPH ,
Vineet Arora, MD, MAPP and David Meltzer, MD, PhD
Research Objective:
Studies in a variety of clinical settings have shown that Black patients have poor functional outcomes compared to their White counterparts. Physical therapy (PT) is an invaluable tool for improving functional outcomes including hospitalization-associated disability and physical deconditioning. However, Black patients in surgical settings are less likely to be offered post-acute physical rehabilitation and older Black patients have lower odds of receiving rehabilitation services in inpatient, outpatient, and home-based settings. It remains unknown whether racial differences in post-acute rehabilitation referral and utilization are affected by social risk in patients hospitalized for acute medical illness. We aimed to assess racial differences in post-acute rehabilitation referral and utilization and whether social disadvantage affects this difference.
Study Design:
Cross-sectional study at a large tertiary academic hospital. Baseline characteristics were compared using chi-squared or t-tests. Regression analysis was used to test for a) the association of Black race with PT discharge recommendations, and b) Among those recommended for discharge to a post-acute care (PAC), the association of Black race with discharge disposition controlling for age, sex, length of stay, admission
mobility score, mobility change (difference in admission and discharge mobility scores), social disadvantage at the neighborhood level as measured by the Area Deprivation Index (ADI), and insurance type. We performed subanalyses by age (< 65 vs ≥ 65), functional impairment on admission, and social disadvantage (high vs low).
Population Studied:
Patients admitted > 48 hours on inpatient medicine services between 1/1/18 – 5/6/22
Principal Findings:
Of the 10,647 inpatient admissions analyzed, (82%) were Black. Black patients were younger (61 vs 62 years old), more likely to be male (53% vs 42%), to reside in a neighborhood with high social disadvantage (37% vs 13%), to have public insurance (92% vs. 67%), and had lower mobility scores at admission (18 vs 19) and discharge (19 vs 20).
After adjustment, Black race was associated with lower odds of discharge to a PAC facility [OR 0.80, 95% CI (0.69 – 0.92)]. Black race was not statistically significantly associated with recommendation for discharge to a PAC facility but was associated with reduced odds of discharge to a PAC facility among those recommended for PAC [OR 0.53, 95% CI (0.41, 0.67)]. The effect held for those < 65 [OR 0.50, 95% CI (0.31, 0.81)], 65+ [OR 0.53, 95% CI (0.40, 0.71)], and those living in the
neighborhoods with the least social disadvantage [OR 0.47, 95% CI (0.32, 0.69)]. There was not a statistically significant association between Black race and discharge to PAC when recommended in those with the most social disadvantage.
Odds of Discharge to PAC for Black Patients
Odds for PAC Discharge Recommendation for Black Patients
Odds of Discharge to PAC for Black Patients
(Among Patients Recommended for DC to PAC)
Conclusions:
Given that Black patients are at risk for poor functional outcomes, their appropriate discharge disposition is especially important for functional recovery after hospitalization for acute medical illness. Our findings show that Black patients are less likely to discharge to a PAC facility except for those with the most social disadvantage.
Implications for Policy or Practice:
Clinicians creating discharge protocols should consider these disparities to help facilitate discharge to a post-acute care facility for physical rehabilitation when it has been recommended for Black patients hospitalized with acute medical illness.